
Peter Chappell’s AIDS Remedy PC1
Our field study in Africa has been published
Background story
I’ve always found off-the-wall therapies interesting because, historically, scientific innovations and new findings have very often come from the fringes of the mainstream. Not always, but very often. That’s why I became interested in homeopathy when friends and colleagues dragged me to Dr Köhler’s legendary homeopathy lectures during my student days. At the time I thought: This is so crazy, if it’s true, then it’s revolutionary. As a result, I became scientifically involved with homeopathy. I did some drug trials and clinical research and then, after about 10 years of intensive research, 3 books [1-3], a series of peer-reviewed papers [4-10], extensive work on placebo effects [11-15], I realized: Yes, something is happening that is beyond random fluctuations, but that we do not understand in any way and certainly cannot explain with the conventional causal models of science [16]. I have tried to make this tangible with the scientific models currently available, but I still don’t know whether that actually leads anywhere [17].
While my hot homeopathic research period was cooling down in the early 2000s, I was approached by Harry van der Zee, a Dutch homeopathic doctor. He wanted to replicate our headache study, but better than us. That study is one of the studies in the homeopathic database that found by far the worst effect for homeopathy [7, 10]. I invited Harry round. We spent a few days together and cooked up the supposedly unbeatable design. Harry went home, did a pilot study, which turned out to be what I predicted, not what he expected. And because there was no funding, nothing came of it in the end.
Peter Chappell and PC1
But we remained friends. Years later, he put Peter Chappell in touch with me. Peter Chappell, who died last year, was an English homeopath who worked as an electrical engineer in his earlier life. His inventions included magnetic strips on plastic money cards, as he once told me. Peter Chappell worked as a classical homeopath for several years and also went to Africa for a while, where he treated people with AIDS. It was there that he apparently had the idea that homeopathy could be made even simpler. He looked at the totality of the symptoms of a clinical picture, e.g. how AIDS manifests itself in Africa. And put this „information“ into a bottle of water. He didn’t say exactly how. But I suspect it is simply an intentional act in which this „information“ is put into a bottle of water with great focus and concentration and probably also a benevolent, healing intention. He later told friends: The remedies were created by making an intense request to the „source“ to produce a simillimum, i.e. a remedy that was as homoeopathically suitable as possible. He apparently perceived this „source“ as a kind of transcendental reality that was both within and beyond him.
This is very similar to the production of homeopathic remedies and Bach flowers, except that in Peter Chappell’s case there was no pharmaceutical preparation and no placing of flowers in the sun, but everything was purely intentional. Peter Chappell developed such remedies for various diseases, but the first was the one against AIDS in Africa, PC1 (for Peter Chappell remedy 1).
AIDS in Africa is more than the result of an infection with the HIV retrovirus. It is a conglomeration of opportunistic infections that can also thrive on the basis of a deficiency-induced weakness of the immune system and contribute to the clinical picture of AIDS. That’s why I say „AIDS in Africa“, because experience has shown that the same drug PC1 does not work so well for AIDS patients in Western countries. But it obviously does in Africa. Peter Chappell developed a different drug for AIDS in Western countries.
Amma Resonance Healing Foundation
In Africa there have been homeopathic treatment centres there since the 2000s. And the Amma Resonance Healing Foundation (ARHF), which Harry van der Zee has since set up, distributes the PC1 remedy there. It is produced in England and Holland, purchased by the ARHF at cost price on a donation basis and distributed in Africa. On the ARHF website you can find all kinds of information about this, including a film showing the actual use of PC1 in Africa.
Years ago, this logistics gave rise to the desire to evaluate the effectiveness of PC1. I took part in a planning meeting and agreed to analyse the data – should there ever be any – and also helped to develop a research protocol. And indeed, a few years ago I received a corresponding data set, the accuracy of which was vouched for by Harry van der Zee, who accompanied and monitored the study on site in Africa. Now, after much toing and froing, the study has finally been published [18].
The study
As there was no data available apart from systematic case reports and observations in the field, Harry and his team decided to organize a naturalistic study in which the groups were based on local choices. Word has got around in Africa that antiretroviral drugs are not always well tolerated and produce a range of side effects. This is why some people do not want to take these drugs. They were offered PC1. All those who wanted antiretroviral drugs were given them. And some of them also wanted PC1, i.e. the full programme.
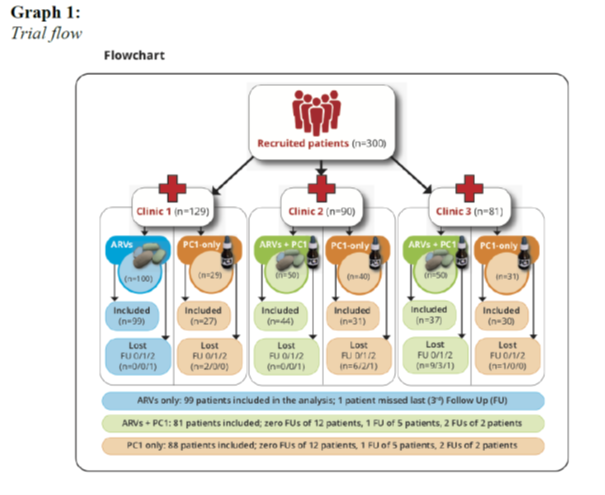
The study was conducted in Kenya, a country that reports the highest number of AIDS cases worldwide. Three different specialized AIDS clinics took part in the study and enrolled patients. The protocol defined that only newly diagnosed AIDS patients who had undergone standard diagnostics (CD4 count, viral load) at baseline should be enrolled. All patients were offered antiretroviral drugs (ARVs). The ARVs distributed there were Abacavir, Lamuvidine and Efavirenz in children and adolescents and Tenofovir in older patients. In one of the three clinics, either ARVs or PC1 were given. In two clinics, patients were offered PC1 in addition to ARVs. In one clinic, patients received ARVs. This was intended as a control. Only if these patients refused the ARVs did they only receive PC1. In this respect, we therefore have a wide spread of treatment protocols and clinics.
PC1 is kept in larger bottles like a homeopathic remedy, and globules are then impregnated with the liquid. For the study, the patients were given a 20ml dropper bottle in which a globule of PC1 was dissolved in mineral water with 20% medical alcohol (the alcohol is necessary to preserve the liquid and prevent unwanted bacterial growth). Patients were supposed to drink one sip per day and shake the bottle beforehand.
The study organization and patient distribution is shown in Figure 1:

A total of 300 patients were included, of which 268 patients could be analysed. Data was missing from the other 32. This was probably due to the fact that the patients had to come to the clinic twice a month to collect their medication. The clinical data was also collected and entered on this occasion. The patients often had to walk very long distances. Some of these were impassable due to rain, and there was apparently also unrest in some parts of the country. Some patients had also entered incorrect telephone numbers and addresses so that they could no longer be contacted. But in my view, a drop-out rate of around 10% in a field study in Africa is a good result and speaks volumes for the local organization.
The Kenyan national protocol stipulates that CD4 count is only measured at the beginning of the diagnosis and viral load every 6 months. In this study, both were measured at the beginning and a blood sample was taken again after 6 months to determine these parameters. In addition, appetite, weight gain or loss, fatigue and weakness were recorded as clinical parameters at each clinic visit.
I carried out the statistical analysis using very robust non-parametric methods. These are methods that make no distributional assumptions about the underlying data distribution and are therefore always applicable. I summarize the most important data in Table 1; the full data can be viewed in our publication.
CD4 count increased more under PC1 than in the other groups, and the viral load decreased. The clinical parameters (weight, appetite, fatigue, weakness) also improved clearly and significantly. The pattern was clear: the patients in the PC1 group improved more in the objective parameters than those in the ARV+PC1 group, who in turn were better than the patients in the ARV group.
One could now assume that this was due to the fact that the patients who only received ARVs were the ones with the greater disease burden. On the contrary, those who received only ARVs were initially less clinically burdened, had better initial data in CD4 count and viral load, while the group that received only PC1 was the one with the worst initial values (original table in our publication).
| ARVs only | ARVs + PC1 | PC1 only | |
| CD4 count increase | 2,48 % | 7,37 % | 19,81 % |
| Viral load decrease | 43,63 % | 43,61 % | 53,35 % |
| Weight gain | 3,28 % | 6,64 % | 8,44 % |
| Appetite (difference)* | 0,63 (0,92) | 1,10 (0,72) | 1,02 (0,88) |
| Exhaustion (difference)* | 0,32 (0,7) | 1,30 (0,78) | 1,16 (0,84) |
| Weakness (difference)* | 0,13 (0,66) | 1,07 (0,79) | 0,75 (0,97) |
If we look at Table 1, which shows the outcome variables, we can see that in the central, objectively measured parameters CD4 count, viral load and weight, the increases under PC1 are significantly greater than under the combination of ARV+PC1 or ARV alone. These effects are highly significant in the non-parametric statistical test. This pattern is slightly different for the clinical variables because the group that received both drugs describes the greater change. But here, too, the PC1 group is far superior to the ARV group. Anyone who has looked at my method blogs on effect size calculation (https://harald-walach.info/methodology-for-beginners/13-power-analysis-the-magic-of-statistics/ https://harald-walach.info/methodology-for-beginners/14-tamiflu-the-biggest-theft-in-history/ https://harald-walach.info/23-how-do-meta-analyses-actually-work/) can now divide the mean difference by the standard deviation and obtain the effect size d. For the clinical variables, these effect sizes are between 0.19 and 0.78 for ARVs, 1.1 to 1.78 for ARVs+PC1 and 0.6 to 1.5 for PC1.
The effect sizes for the active groups ARV+PC1 and PC1 are therefore clinically large to very large and thus definitely significant. For the ARV group, they are still relatively large, but significantly smaller.
Overall, this shows that PC1 is apparently not only not inferior to ARVs, but clearly superior. Apparently, a combination of these two treatments also makes clinical sense.
This data must, of course, be viewed against the background of its potential problems.
Possible sources of error
The study was naturalistic. This means that the groups were formed by the choice of patients and/or doctors, and not by chance. It also means that the observed effects could of course have been caused by third variables that have not yet been described further as well. As already mentioned, it is very unlikely that this was due to the fact that the patients in the PC1 group were less severely ill. This is because the clinical values of this group were worse in all the parameters recorded. At most, it could be that the values deviated more strongly from the expected value in the second measurement, i.e. a statistical regression towards the centre took place. But it seems to me that such a large and consistent deviation cannot be explained by a statistical artefact. Especially as a one-year follow-up was also carried out on 32 patients in the PC1 group, which confirms the positive trend. This is because the improvement continued there.
The lack of blinding is also a shortcoming of this study. Given the fact that patients and practitioners knew who was treated and how, it is possible that a bias occurred. This could work in favour of PC1, namely when patients or practitioners are positively affected by the treatment. But of course it could also have a different effect. We simply do not know. However, the fact that the laboratory values were analysed in laboratories that had no knowledge of the treatment and therefore simply carried out measurements that were practically blinded speaks against this. The larger effect sizes of the ARV+PC1 group only in the clinical parameters seem to me to be an indication of bias. This is because these were collected openly and everyone knew that the patients received two treatments. As we know, two is more than one treatment. So better values.
Some might say: at least the people in the PC1 group drank a mouthful more water a day than the others. Rather unlikely. Because we are talking about 5 drops a day. Perhaps this would also have to be checked in a good study. But that would be the ultimate embarrassment if a mouthful of water was better than ARVs.
And for those with a knack for statistics: multiple testing is not the problem. I did tests for a total of six variables. But the significance levels were so high that I could have tested a whole battalion of variables and the significance would have remained even after correcting for 100 variables. See the original publication.
Confounding variables cannot be ruled out in naturalistic studies. Therefore, only a randomized study that randomly assigns all patients from the outset would provide certainty. The relevant information is now available. It is to be hoped that the planners of this study will find a way to corroborate these data in a methodologically clean randomized study.
Intention in a bottle – Conflict of Interest Statement
Apparently, as this study shows, a therapeutic intention can be bottled and distributed for the benefit of those it is intended to help. In any case, side effects were not observed and have never been reported in previous observations.
It remains to be mentioned: All those involved, Harry van der Zee, Peter Chappell and I, are working in this context on a non-profit basis. I have made my time available free of charge, as has Harry. The medicines are produced by a pharmacy from which the Amma Resonance Healing Foundation buys them and distributes them free of charge in Africa. This is done by means of donations. The staff who worked on site for the study were financed by the state. The ethics committee of the University of Northampton, where I was at the time, examined this study and categorized it as ethically unproblematic.
So we have a negative conflict of interest. If this treatment becomes established in Africa or proves to be effective in further studies, then we’ll be getting a hammering from those whose ARV skins are swimming away. But I’m already used to that.
Sources and literature
- Walach, H., Wissenschaftliche Homöopathische Arzneimittelprüfung. Doppelblinde Crossover-Studie einer homöopathischen Hochpotenz gegen Placebo. 1992, Heidelberg: Haug.
- Walach, H., Homöopathie als Basistherapie. Plädoyer für die wissenschaftliche Ernsthaftigkeit der Homöopathie. 1986, Heidelberg: Haug.
- Walach, H., Wissenschaftliche Untersuchungen zur Homöopathie. Die Münchener Kopfschmerzstudie -Arzneimittelprüfungen mit Belladonna. 2000, Essen: KVC Verlag.
- Walach, H., Die Untersuchung der Homöopathie durch das Reichsgesundheitsamt 1936 – 1939. Zeitschrift für Klassische Homöopathie, 1990. 34: p. 252-259.
- Walach, H., et al., Research on homeopathy: State of the art. Journal of Alternative and Complementary Medicine, 2005. 11: p. 813-829.
- Walach, H., et al., The effects of homeopathic belladonna 30CH in healthy volunteers – a randomized, double-blind experiment. Journal of Psychosomatic Research, 2001. 50: p. 155-160.
- Walach, H., et al., The long-term effects of homeopathic treatment of chronic headaches: One year follow-up. Cephalalgia, 2000. 20: p. 835-837.
- Walach, H., Homoeopathy as Semiotic. Semiotica, 1991. 83: p. 81-95.
- Walach, H., Does a highly diluted homoeopathic drug act as a placebo in healthy volunteers? Experimental study of Belladonna C30. Journal of Psychosomatic Research, 1993. 37: p. 851-860.
- Walach, H., et al., Classical homoeopathic treatment of chronic headaches. A double-blind, randomized, placebo-controlled study. Cephalalgia, 1997. 17: p. 119-126.
- Walach, H. and W.B. Jonas, Placebo research: The evidence base for harnessing self-healing capacities. Journal of Alternative and Complementary Medicine, 2004. 10(Suppl. 1): p. S103-S112.
- Walach, H., et al., Homeopathic proving symptoms: result of a local,non-local, or placebo process? A blinded, placebo-controlled pilot study. Homeopathy, 2004. 93: p. 179-185.
- Walach, H., Placebo and placebo effects – a concise review. Focus on Alternative and Complementary Therapies, 2003. 8: p. 178-187.
- Walach, H. and C. Sadaghiani, Plazebo und Plazebo-Effekte: Eine Bestandsaufnahme. Psychotherapie, Psychosomatik, medizinische Psychologie, 2002. 52: p. 332-342.
- Walach, H., The efficacy paradox in randomized controlled trials of CAM and elsewhere: Beware of the placebo trap. Journal of Alternative & Complementary Medicine, 2001. 7: p. 213-218.
- Walach, H., Magic of signs: a non-local interpretation of homeopathy. British Homeopathic Journal, 2000. 89: p. 127-140.
- Walach, H., Entanglement model of homeopathy as an example of generalizsed entanglement predicted by Weak Quantum Theory. Forschende Komplementärmedizin und Klassische Naturheilkunde, 2003. 10: p. 192-200.
- van der Zee, H. and H. Walach, Novel immune supportive treatment of HIV/AIDS: comparative outcomes study in rural clinics in Africa. International Journal of Healing and Caring, 2024. 24(1): p. 18-43.