The German Bundestag petition calling for a review of the Measles Protection Act is online
Anyone who hasn’t been asleep over the past few years will have noticed: the signs point to coercion and state paternalism. Everywhere. But especially in the healthcare sector. The SARS-CoV-2 pandemic was a vast funnel designed to drive the majority of people towards untested and, as we now know, dangerous genetic prevention technologies, which politicians euphemistically sold to us as ‘vaccinations’. The promises were all hollow, not to say outright lies. From Germany’s Merkel’s “The pandemic will be over once we have the vaccine” to Health Ministers‘ Spahn and Lauterbach’s “effective and safe”.
During this pandemic, on 10 February 2020, a new Measles Protection Act was enacted, which came into force on 1 March 2020, conveniently at a time when nobody was really paying attention. The draft dates from September 2019, and anyone familiar with ministerial bureaucracy knows that something like this must have been hatched some time beforehand so that it could then be presented to parliament as a draft.
The core of this law is the requirement for nursery school children to provide proof of measles vaccination so that they can attend nursery school or a childcare centre. Immunity to measles can also be demonstrated by antibody titers, i.e., by the fact that a child has already had measles (see). As compulsory schooling takes precedence in Germany, checks may still be carried out and a missing vaccination certificate reported to the health authority, but the authorities are not permitted to prevent the child from attending school. Once compulsory schooling has ended, i.e., for secondary and further education, this may become an issue again.
In effect, therefore, the requirement to provide proof of a measles vaccination amounts to the introduction of a compulsory measles vaccination.
In Germany, virtually no single-dose vaccines are left in stock or available to order. To my knowledge, they are still available, in Switzerland for example, and if one is determined and pays for them oneself, but not as a standard medicine. Consequently, the measles vaccine is only ever available as part of a triple pack with mumps and rubella (MMR vaccine). That is why this requirement to provide proof is, in effect, a compulsory triple vaccination. One could say, even if it is legally incorrect, it is a pragmatic form of compulsory vaccination. You can only avoid this compulsory vaccination if a doctor certifies that you are medically unfit for vaccination, but this must also be recognised by the public health authority or the relevant institutions. In the worst-case scenario, parents must brace themselves for a legal gauntlet.
A child may be medically unfit for vaccination if, for example, an allergy or an adverse reaction has already been identified following another vaccination. This happens quite frequently. Scientifically speaking, an inability to be vaccinated should actually be assumed in every case. This is because the risk of suffering harm from a measles vaccination is many times higher than from measles itself.
The risk of a vaccination is more than 2,500 times higher than the risk of a measles complication
My colleague Dr Andreas Sönnichsen has calculated this:
According to official data from the RKI, there were only 233 cases of measles in 2025 amongst a population of 83 million. So the risk of contracting measles is 0.00028% and 0.0004% if one takes the average figure from previous years as a basis.
As serious complications occur in fewer than one in 1,000 people with measles, the risk of a serious measles complication is a further three decimal places lower. Even if this risk is multiplied by life expectancy, the lifetime risk of a serious measles complication is approximately 0.00003%.
Based on official data on reported side effects from the measles vaccine, Andreas Sönnichsen calculates that the risk of suffering vaccine-related harm is 0.08%. This means the risk of suffering serious harm from the vaccine is 2,666 times higher than the risk of suffering harm from measles itself.
Because the risk of this vaccination is more than 2,000 times greater than the risk of the disease itself, every child is, ipso facto, actually ineligible for vaccination. For any medical intervention, particularly on a healthy body, requires that the benefit outweighs the risk. If this is not the case, according to standard medical ethics, the intervention must not be carried out.
This is also the reason why the association “Doctors and Scientists for Health, Freedom and Democracy – MWGFD e. V.”, of which I am currently the chairman, held a press symposium on this topic some time ago, at which these data were published; you can watch the videos on our website. There is further information on this on the website.
As a first step, my colleague Dr Ronald Weikl, together with others, has submitted a petition to the Bundestag with the aim of repealing this Measles Protection Act. We have already collected more than 8,000 signatures within a few days. By 4 June 2026, 30,000 signatures must be submitted in order to reach the quorum and for the petition to be presented to the Bundestag’s Petitions Committee. (Only German citizens can sign.)
If you’d like to hear a few more arguments as to why this – and, frankly, any – compulsory vaccination is nonsense, you can read on here. Before you do, a very important…
distinction: compulsion and voluntary action
My arguments against a mandatory vaccination scheme are not arguments against vaccinations per se, although I must admit I am rather sceptical about the benefits of vaccinations. But I am not a die-hard anti-vaxxer. We have had our four children vaccinated against certain diseases, and I myself have also received the odd vaccination. But you don’t have to be against vaccinations to be against a mandate for vaccination or against compulsory vaccinations.
My arguments are directed against a mandate and against state coercion. I am committed to liberal and conservative values. This means: the state should only interfere in citizens’ lives where it is truly necessary and otherwise keep as far back as possible. Health is the area that should be regulated as little as possible, because this is where the individual’s free choice to live and die in a way that is consistent with their values is manifested.
The supposed threat posed by measles and other infectious diseases
The compulsory measles vaccination stems from the repeated assumption that measles and other infectious diseases pose a major threat. This perception is the result of media scaremongering and pharmaceutical interests. For nothing is more lucrative than the value created by healthy bodies. These are constantly being born anew and thus represent a continuous source of value creation for vaccine manufacturers. With every new infectious disease discovered and every new vaccine, this potential for value creation increases. Since drugs have now been developed for most diseases and diseases are finite, it is far more lucrative to exploit the infinitely renewable ‘raw material of healthy bodies.’ And that is precisely what we are seeing at present: more and more, ever newer, ever more expensive vaccines are being introduced.
This can be achieved by spreading the message through the media about how dangerous these diseases are. We saw how this works during the SARS-CoV-2 pandemic. People are restricted by lockdowns, mandatory testing, and other forms of harassment. They are offered a way out: the ‘vaccine,’ and, bang, everyone jumps through the hoops, or at least the vast majority. That is enough.
In the case of measles, the big bogeymen are “measles death” and “measles encephalitis”. My medical colleagues, who have practiced for a lifetime – you can listen to this in our measles symposium – say the following: measles encephalitis is primarily an iatrogenic problem, i.e. one induced by incorrect treatment. It arises when the fever a child develops from measles is reduced too drastically. This can allow an opportunistic infection to spread or lead to encephalitis.
The data
Now, let’s take a look at the data. I have included two graphs below. The first is taken from official statistics from the Centers for Disease Control (CDC) [1]. The second is from the CDC’s ‘Wonder’ database, where you can compile your own data, which is what I have done.
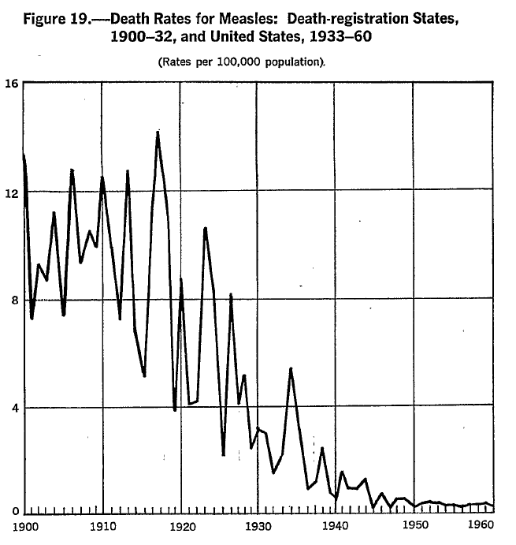
Two things are evident from Figure 1, which shows the official US mortality data for measles deaths:
- The mortality data, standardised to 100,000 inhabitants, were already low at the beginning of the 20th century, namely a maximum of 15 per 100,000 inhabitants, or 0.015% or 0.15 per mille, and then fell to below 1 per 100,000.
- The vaccinations introduced after 1963 (inactivated vaccine) and 1973 (live vaccine) could no longer make any significant difference to the mortality figures, because these were already at rock bottom. In statistics, this is known as the ‘floor effect’.
These data reflect a very well-known phenomenon that Thomas McKeown had already demonstrated in 1976 using hard data from Wales [2, 3]: all infectious diseases, except for polio, were already declining before the introduction of any vaccines, indeed even before the exact pathogens were known.
The reasons for this are simple:
- Improved hygiene,
- the introduction of sewage and drainage systems – in London, for example, after 1858
- the separation of sewage discharge into rivers from the extraction of drinking water,
- better living conditions,
- better food,
- more hygienic conditions in food preparation, e.g., through the ban on milk from sick cows and the pasteurisation of milk, etc.
Figure 1 only extends to the early 1960s because the statistical text was published in 1968. I have therefore added the data from 1968 to 1997 based on the Wonder database (after 1997 the values are ‘0’, so the data does not continue) and presented it in Figure 2. These are unstandardised raw data because the case numbers are so low. Vaccines were available after 1963 and 1973, but the measles vaccination became compulsory in 1978.
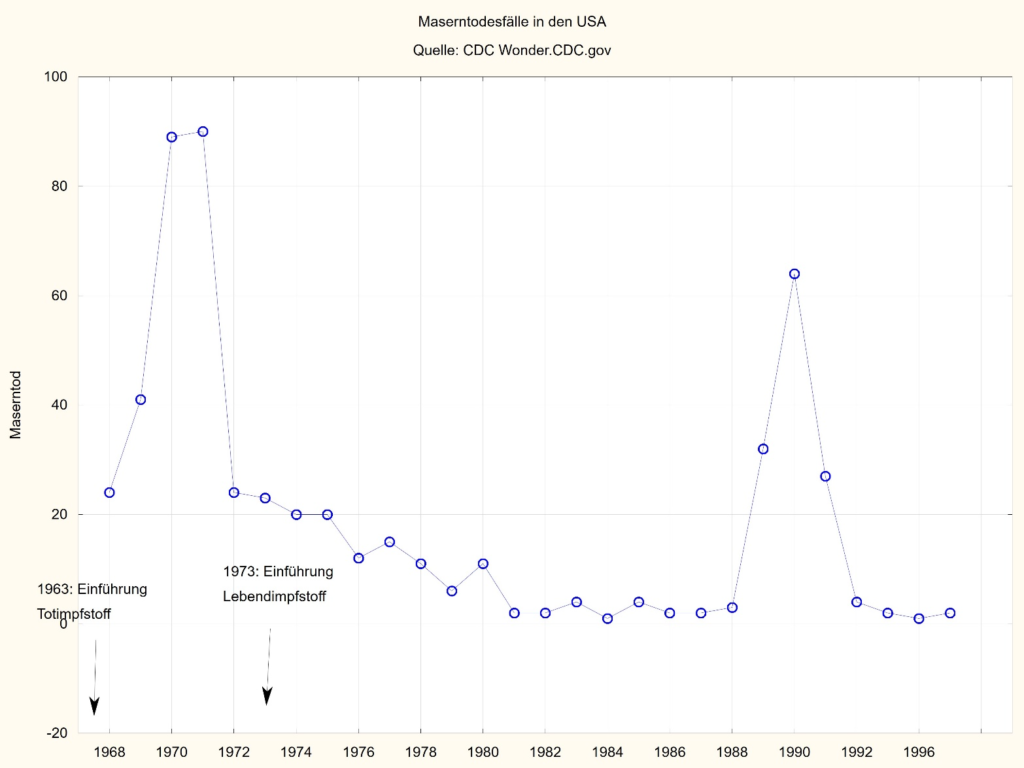
As can be seen from Figures 1 and 2: Measles vaccinations, their availability, and the mandatory vaccination requirement from 1978 onwards had no discernible effect on measles deaths. There were very few to begin with, namely fewer than 100, which is barely noticeable in a population of 200 to 270 million between 1968 and 1997.
The large outlier in 1980 could be attributed to several measles outbreaks that were detected at the time despite high vaccination coverage. For example, a measles outbreak was reported in 1987 at a school near Boston. 97% of the children there had been vaccinated. 27 children had measles, and only three of these were unvaccinated. The sole factor determining whether a child contracted measles or not was not whether they had been vaccinated, but how close they had been to an infected child [4]. Whether or not measles outbreaks occur, therefore, seems to have less to do with whether people are vaccinated or not, and more to do with factors that we do not yet understand.
In 2026, the RKI described a measles outbreak from 2024 at a reception centre in Berlin-Tegel, where refugees from Ukraine were being housed [5]. 52 people contracted measles, 31% of whom were verifiably vaccinated. The others are likely to have been vaccinated twice as children in Ukraine, though this could not be verified; it is merely an assumption based on local practice there. Eighteen of the unvaccinated individuals were vaccinated on site, but this did not prevent the infection. Here too, proximity was apparently the main driver of the infection.
In 2021, Di Pietrantonj and colleagues presented a systematic Cochrane review of all relevant studies on vaccinations against measles, mumps, and rubella (as these are always administered together) [6]. The effectiveness of the measles vaccine is estimated at 95%. If one examines the data more closely, which is what we are currently doing, one sees that there are no truly good randomised placebo-controlled trials. Most of the data is older and consists of cohort studies and observational studies. Consequently, the certainty with which these statements are made is only ‘moderate’ to ‘low’.
In Cochrane jargon, this means: there are no truly good studies to substantiate this.
The authors state that there is an association between the vaccine against certain strains of mumps and meningitis; in other words, the vaccine can trigger meningitis. The occurrence of febrile convulsions in one in approximately 1,500 cases is also documented. The association with other side effects (encephalitis, inflammatory bowel disease, autism) cannot be either confirmed or ruled out by this review because the data is of poor quality. Further studies are therefore required.
So that is the state of the art. To put it plainly, we do not actually know enough. What we do know is that side effects occur much more frequently than serious complications from the disease itself (see above). We also know that serious complications from measles are very rare with proper treatment. Proper treatment would involve mild fever reduction, for example, through calf compresses and good care, and no aggressive fever reduction. We also know that natural immunity is far superior and lasts longer than that induced by vaccination. What we do not know is what secondary conditions arise from the child being deprived of the maturation of the immune system through exposure to a childhood illness. We know, for example, that children from the countryside, who are exposed to a much wider range of allergens and pathogens, are healthier and suffer less frequently from hay fever and asthma [7]. It is therefore not always beneficial to try to prevent everything that could be dangerous. Ultimately, this very attitude could prove dangerous, as it prevents our immune system from dealing with threats at a young age, when it is highly adaptable and malleable.
Conclusion
If one looks at the hard data, the following becomes apparent.
- Measles is no longer a deadly disease. This is because our standards of hygiene, living, and nutrition have helped to ensure that the danger of infectious diseases has long since been averted.
- The risk of suffering harm from a measles vaccination is far greater than from the disease itself.
- This effectively undermines the basis for any state coercive measure ipso facto.
- Therefore, the Measles Protection Act should be repealed without replacement
- There is a danger that the population will gradually become accustomed to state paternalism and that the state, through more or less corrupt or ideologically blinded ‘experts’, will become a stooge for an industry that has discovered the healthy body as a new arena for value creation.
- We can assume that this is already in the pipeline with the new modRNA platform. More on that another time.
References
- Grove RD, Hetzel AM. Vital statistics rates in the United States, 1940-1960. Washington, D.C.: U.S. Department of Health, Education, and Welfare, Public Health Service, National Center for Health Statistics 1968.
- McKeown T. Die Bedeutung der Medizin: Traum, Trugbild oder Nemesis? Frankfurt: Suhrkamp; 1982; orig. 1976 1982/ /.
- McKeown T. The Role of Medicine: Dream, Mirage, or Nemesis? London: The Nuffield Trust; 1976.
- Nkowane BM, Bart SW, Orenstein WA, Baltier M. Measles outbreak in a vaccinated school population: epidemiology, chains of transmission and the role of vaccine failures. American Journal of Public Health. 1987;77(4):434-8. doi: https:/doi.org/10.2105/ajph.77.4.434. PubMed PMID: 3826461.
- Sarma N, Martín-Sánchez M, Larscheid P, Möller-Kutzki M, Ruscher C, Bitzegeio J, et al. Masernausbruch im Ankunftszentrum für geflüchtete Menschen in Berlin Tegel, März-Juli 2024. Epidemiologisches Bulletin. 2026;(5):19-32. doi: https:/doi.org/10.25646/13685.
- Di Pietrantonj C, Rivetti A, Marchione P, Debalini MG, Demicheli V. Vaccines for measles, mumps, rubella, and varicella in children. Cochrane Database of Systematic Reviews. 2021;(11). doi: https:/doi.org/10.1002/14651858.CD004407.pub5. PubMed PMID: CD004407.
- Gassner-Bachmann M, Wüthrich B. Bauernkinder leiden seltener an Heuschnupfen und Asthma. Deutsche Medizinische Wochenschrift. 2000;125:924-31.